
Wellness Wednesday Oct 9
Hi Everyone,
Last week, we concluded a conversation about non-oral pharmacological care (topicals) for pain. A couple of questions were asked, so I would like to take this week and address them.
The first question referred to inflammation and being able to address it with topicals, and the second question was concerning CBD (topicals). In this week’s Wellness Wednesday, I will try to answer the first questions and then begin a discussion of CBD.
Inflammation
Chances are you have experienced the effects of inflammation on your body at some time. While inflammation often has a bad reputation, it may be a healthy response to challenges your body faces, such as infection, illness, or injury. Acute inflammation, for example, is a normal protective response to injury.
However, inflammation can become your enemy if it is causing your body to overreact to stressors, creating a chronic, continuing natural inflammation response. Your lifestyle habits, including diet, nutrition (omega fatty acids especially), and exercise, may affect the way your body addresses those challenges.
The idea of using “anti-inflammatory” medication, such as NSAIDs to address inflammation, has begun to lose favor, because if inflammation is artificially interrupted or blocked, healing is blocked AND you could also suffer the side effects of these medications (See Part 1 – Options to Opioids).
Essential oils and inflammation balancing
Aside from the active ingredients of the topical, additional ingredients can augment the desired effect without disrupting healing.
- Essential Oils for topical Pain relief
- Some of the most impressive essential oils for pain include arnica, marjoram, sandalwood, fennel, rose, bergamot, lavender, juniper, , cayenne and clove Essential oils rich in capsaicin and other anti-inflammatory compounds, make potent allies in the fight against pain.
- Essential Oils for Inflammation
- If you are looking for essential oils for inflammation, some of your best options include frankincense, rose, eucalyptus, clove, thyme, bergamot, patchouli, sandalwood, spruce, chamomile, rosemary and peppermint, among capsaicin and many others. , making it a potent ally in the fight against pain.
- Essential Oils for Inflammation and Swelling
- A top recommendations is to use Ginger oil for swelling…thyme, and Eucalyptus also reduce swelling.
- Essential Oils for Bruising
- Considered one of the best essential oil for bruises, rosemary is often a key ingredient in natural bruise remedies. Scientific evidence notes that several bioactive compounds may be responsible for the main benefits of rosemary essential oil, which include natural pain relief and anti-swelling activity.
- You can also mix powdered turmeric with Frankincense to hit all three: inflammation, bruising and pain.
What about Topicals containing CBD?
GREAT Question….but not an easy answer! A lot of people claim it helps and yet there are an equal number that claim it didn’t work for them.
To understand CBD and its topical or oral impact on the body, a more thorough discussion needs to happen. We will need to define CBD, sources, active ingredients, current processing/uses, anecdotal vs. scientific results, regulations, etc. This will ultimately take more than just one Wellness Wednesday (i.e. a mini-series of discussions).
Thanks for reading!
Dr. Larry Sharp, D.C., Associate Professor
Department of Biology
McMurry University
1 McMurry Station | # 368 | Abilene, Tx 79697
(o) 325-793-3871
Wellness Wednesday Oct 2
Hi Everyone,
Last week, we started a conversation about non-oral pharmacological care for pain in Part 1 of the two-part series, “Topical Analgesics: Options to Opioids”.
One question comes to mind when looking at topicals…Are they really a healthier alternative to Pain Relief?
In December 2017, the journal Postgraduate Medicine published a study involving 121 patients who were taking opioids for pain. After engaging in treatment with topical analgesics for a period of three months, 49 percent of the patients had completely discontinued opioid use. The same subjects were also assessed at the six-month mark and researchers found that 56 percent of the study participants reported that they no longer used opiates. Perhaps better yet, they were also experiencing lower levels of pain.
Another study, this one in the Journal of Pain Research, found similar results. In this case, 631 patients were assessed three months after topical use and researchers found that those using topicals showed de-escalated use of pain medications. This is opposite of what they found in the control group as those subjects, on average, actually escalated their pain medication use.
This week, Part 2, we will try to tie the science (discussed last week) to how, why, and when to use topical analgesics.
How to Use Topicals – Part 2
In addition to identifying which active ingredients can be used in topical analgesics, as well as the amounts deemed to be effective while still remaining safe, the Food and Drug Administration places fairly strict guidelines regarding directions of use to be placed on topical packaging. For instance, if the topical contains an active ingredient, the label must identify the product as an “external analgesic,” “topical analgesic,” or “pain-relieving” lotion, ointment, or cream, whichever the case may be. It must also contain the appropriate age and application statements.
While this is a great starting point on the proper use of topicals, there is additional advice that can help you gain the most benefits possible from these types of products. This begins with understanding a few basic principles.
Basic Topical Use Principles
Mucous membranes such as eyes, nasal passages, and genitals are particularly sensitive to the active ingredients in topical analgesics. Therefore, it may be best to use gloves when applying these products. And if gloves are NOT worn, wash your hands extremely well post treatments so as not to upset these areas by inadvertently getting the topicals in or on them. (Voice of experience talking now: capsaicin is extremely hard to wash off your hands….if you remove your contacts after incompletely removing that active ingredient, you will pay the price for a while…wish I had worn gloves!).
Before applying the topical, wash the area to be treated with soap and water. This helps to remove any excess dirt, oil buildup, or previously applied lotions or topicals – This will insure there are no barriers between the ointment and your skin.
When rubbing in the topical, pay close attention to the directions provided for that particular brand. For instance, some topicals instruct users to only rub the product into the skin for a few seconds while others state to rub longer. Last week, we talked about the transient receptor receptor channels (TRPs), commonly referred to as ion channels, and their sensitivity to pressure. This means that the action of rubbing a topical on the skin can play a role in the temporary role in pain relief. Knowing how to properly use your specific product line will help you get the most favorable results.
Finally, once the topical is applied, loose-fitting clothes should be worn over the areas of application. This helps prevent irritation or blistering that could potentially occur as a result of the topical’s heat.
The FDA’s Safety Do’s and Don’ts for topicals also recommends not applying bandages on top of areas where topicals have been administered. The FDA also warns that topicals containing active ingredients should also not be applied to areas where there are wounds or damaged skin.
Topical best practice for: Joint and Muscle Pain
If the topical is being used to help relieve joint or muscle pain, use just enough to cover the area of pain. Further, the sensation felt after application will depend on the topical used and the ingredients it contains. (Once again, read the directions to help you get the most favorable result.)
For instance, if a topical containing menthol is used, the patient will likely notice that the area grows cold. However, with topicals containing capsaicin, a warm sensation will become more noticeable. Some products provide both effects, causing the user to first experience a cool feeling followed by a comfortable warmth.
Additionally, cool therapy is beneficial if the injury is newer whereas warm therapy works best for long-term, chronic pain conditions.
If you are struggling with cramping or tight muscles, application of a warming gel can help provide relief.
Regardless of the temperatures noticed, you should begin to experience a reduction in pain within about 10 minutes. This reduction can last from four to six hours. (After a few hours, TRPs will reset themselves, so you will need to reapply the topical.)
Topical recommendations for: Pre- and Post-exercising
Topicals can be extremely beneficial for individuals who live active lifestyles. For example, a warming topical applied prior to exercising can help expedite the warming-up process, potentially minimizing injuries generally associated with working “cold” muscles.
Research has also found that topicals are great for post-exercise as well. Application of a cooling topical to a particular muscle group, after exercise-induced stress, will reduce pain in the same way that ice relieves soreness.
Vasodilation’s role in the process
Vasodilation is the widening of blood vessels that result from relaxation of the muscular walls of the vessels. This allows for greater blood flow, and thus more oxygen and healing nutrients to the injured or damaged area. It is unclear on the mechanism for vasodilation for reducing pain. Some surmise that the warming feeling acts to relax muscles surrounding joints, while others believe that the warming sensation serves as a counter-irritant distracting the user’s pain receptors from the original pain signals.
Regardless of which mechanisms apply, topicals can help restore peripheral vascular function after sustaining exercise-induced muscle injury. Methyl salicylate is one of the more common vasodilators found in topical analgesics.
Topicals and Other Warming and Cooling Products
Under its safety guidelines, the FDA also warns that, when using topicals, it is important to avoid using them with any heat-emitting source, such as “heating pads, hot water bottles or lamps” as this can increase burn risks. This warning should apply to ultrasound devices as well. Furthermore, care should be taken when showering after application of a warming topical as hot water can cause the treated area to become irritated uncomfortably.
And if the skin becomes irritated or starts to feel like it is burning after use, use cider vinegar to “wash over” the treated area.
If the burning continues, the FDA urges that medical attention should be sought
Menthol more effective than ice
When faced with pain – whether chronic or acute – one of the most common recommendations is to ice the pained area. Not only is this good for the pain, but ice also helps reduce swelling and inflammation. Yet, research has found that menthol is potentially more effective with regard to pain relief specifically. In the International Journal of Sports Physical Therapy, participants performed certain exercises to induce delayed muscle soreness in their elbow flexors. Two day later, treatments with ice or a menthol topical were used. Those using a menthol topical reported lower levels of pain AND their elbow flexor contractile force was greater than the group using ice.
If the topical has a cooling agent, it can be used in conjunction with an ice pack without any issues. Application of a cooling topical to a particular muscle group, after exercise-induced stress, will reduce pain in the same way that ice will relieve soreness. In fact, doing so can actually extend the benefits of the topical’s cooling effect.
What Topicals should I consider?
When deciding which topical analgesics to buy, there are many factors to consider, including active ingredients, base, smell, and effectiveness.
Think about these questions as well:
- Does it work for a majority of others? Effectiveness?
- Are there different formulations that fit your needs? Cooling only? Warming only? Combination?
- Does smell matter?
- Is it manufactured in the USA?
- Does the product have a history in the market?
Using active ingredients found in topicals, that have been found to affect certain pain receptors, you can positively impact/overwhelm/override some TRP channels in large and small diameter nerve fibers to ultimately reduce acute and chronic pain!
Dr. Larry Sharp, D.C., Associate Professor
Department of Biology
McMurry University
1 McMurry Station | # 368 | Abilene, Tx 79697
(o) 325-793-3871
Wellness Wednesday Sept 25
Hi Everyone,
While the nation’s attention on the opioid epidemic has heightened, interest in options for non-oral pharmacological care for pain has also increased. This two-part series, “Topical Analgesics: Options to Opioids” will introduce you to topical analgesics, the different types of active ingredients, the science behind their action (Part I), and how to use them (Part II).
Topical Analgesics: Options to Opioids – Part 1
The mainstream health care system is clearly failing those who suffer from acute pain or chronic pain (definition: daily pain lasting at least three months OR pain that lasts six months or more and exists on at least half of those days). Most people start with over-the-counter (OTC) pain remedies before turning to a revolving door of specialists, tests diagnoses, and pharmacological treatments. Whatever the causes – acute or chronic pain from physically demanding jobs, chronic inflammation due to arthritis, muscle recovery from intensive workouts, or for any other reason—the best topical pain relief solutions are within reach.
What exactly are topicals?
Topicals is short for topical analgesics that are FDA regulated products that are applied to the skin to relieve pain. Research has substantiated that it is the active ingredients in these topicals that make them so effective. Research has also supported the notion that joint and musculature injuries (sprains, strains, osteoarthritis, and neuropathic pain) typically respond well to topical use. A prescription usually is not necessary to buy many of the topicals on the market today, though some do require a doctor’s order, if they contain high concentrations of active ingredients.
Why choose topicals over OTC medications?
There are side effects associated with ingesting OTC pain relievers.
- Many studies have shown that these types of products can cause damage to the liver, heart and kidneys.
- Aspirin use has an increased incidence of gastrointestinal bleeding.
- Ibuprofen has numerous adverse reactions including gastrointestinal bleeding, renal failure, heart failure and bronchospasm.
No such side effects result from topical analgesics because they are specific to the application site and do not penetrate into the blood stream, so they do not create issues with the rest of the body.
Navigating Active Ingredients and FDA Regulations
Topicals generally contain active ingredients that are medicines regulated by the FDA. The FDA divides topicals into three active ingredient categories:
- Analgesics, anesthetics, and antipruritic (anti-itch) active ingredients.
- Active ingredients that help relieve pain or itching.
- Includes ingredients such as lidocaine, camphor, and menthol
- Counterirritant active ingredients; and
- Active ingredients that work by causing “irritation or mild inflammation of the skin for the purpose of relieving pain… by stimulating cutaneous receptors.”
- Includes the well-known ingredient of capsaicin
- Combinations of active ingredients.
- Identifies which items from the first two categories can be combined in one medication
NOT covered: CBD (cannibidiol) has not been approved by the FDA for use as an active ingredient for topical pain relief.
Topicals: Mechanisms of Action
Gate control theory
For many years, pain perception was measured by the intensity and degree of tissue damage, until the gate control theory of pain was published. The theory’s premise is that pain messages do not just travel from the nerves to the brain. Instead, there are “nerve gates” that control how much of the message will make it through, ultimately impacting the intensity of the pain felt. If this neurological gate is open, the pain signals are perceived by the brain as being more intense. Conversely, if the neurological gate remains closed, or only partially open, the pain is perceived as less intense. Furthermore, with the right intervention, the messages may not make it through at all.
There are two types of nerve fibers that transmit pain: Type C (thin-diameter) and Type A-delta (large-diameter) fibers. This information is transmitted to two types of cells in the spinal cord: transmission cells, which pass the pain signal on to the brain; AND inhibitory cells, which impede the activity of the transmission cells. Gate control works through a combination of both of these type of fibers.
Type A-delta fibers transmits acute pain such as that from a knife wound or breaking a bone. These nerve signals travel rapidly to the spine because humans must be quickly notified that their injury is serious and has to be addressed immediately.
Type C fibers transmit pain signals more slowly and tend to communicate chronic pain, such as that from arthritis.
Under this theory, You can potentially avoid pain by overriding these fibers, essentially closing the gate so the signal can’t get through and modulate the degree of pain experienced. This is at least partially why treatments related to massage, acupuncture, and TENS units are so effective, because this is what they do. It’s also the reason that topical analgesics work to decrease pain as well. (i.e. A topical can be useful in stimulating a large fiber to close the gate and reduce the pain felt.)
Though the gate control theory provides some explanation for how topicals can help relieve pain, a clearer understanding of their mechanism comes with knowing about TRPs.
What are TRPs and Why are they important?
Residing on the membranes of nerve cells in these fibers are ion channels called Transient Receptor Potential Channels (TRPs). These ion channels are different but all of them regulate the flow of ions such as calcium and sodium into and out of nerve cells, allowing or preventing the transmission of sensory signals, including pain.
There is a subset of TRPs that are sensitive to temperature, a fact that is relevant to the ingredients in topical analgesics:
TRPM8 is sensitive to the cold caused by menthol;
TRPV1 is activated by the heat of capsaicin;
TRPV3 is activated at physiological temperatures between 22 and 40 degrees Centigrade, which results from camphor;
TRPA1 is sensitive to citrus oils; and
Furthermore, some TRPs that mediate strong pain are also sensitive to pressure, which means that the action of rubbing a topical on the skin can play a role in temporary relief. (e.g. when you bump your elbow, you rub it to make the pain better…?)
Blah, blah, blah……What does this really mean?
This means that by using active ingredients, that have been found to affect certain pain receptors, you can positively impact/overwhelm/override some TRP channels to ultimately reduce pain!
- The active ingredient capsaicin “activates TRPV1 receptors” to trigger an influx of cations that overwhelms the receptor and shuts down its transmission of pain for a short period of time.
- Menthol “impacts TRPM8 receptors” to help reduce pain.
- Others believe that active ingredients serve as a counter irritant, distracting the user’s pain receptors from the original pain signal.
- Citrus oils and camphor also impact receptors resulting in less pain; and
- Reduces inflammation. (as they also affect vasodilation)
So……what’s next? Hopefully, you have made it this far in reading about topicals!!!!!
We also need to address vasodilation to help restore peripheral vascular function especially with its pivotal role in helping with any type of tissue injury (i.e reduce pain). Topicals can provide the same type of effect. This is important with their application. “How to Use Topicals” next week will tie all of these components together. Although the mechanisms behind topicals can be somewhat complex, having just a basic understanding makes it easier to understand how they work and how to use them.
Next week: How to Use Topicals
Dr. Larry Sharp, D.C., Associate Professor
Department of Biology
McMurry University
1 McMurry Station | # 368 | Abilene, Tx 79697
(o) 325-793-3871
Wellness Wednesday Sept 18
Hi Everyone,
Okay, back to our planned discussions. This week’s talk is about gluten/gluten sensitivity; then, options to opioids for pain; and followed by a discussion(s) on CBD oils. I hope you enjoy this and please let me know if you have other topics that you want to be discussed.
Consuming even minimal amounts of gluten from one of the hidden sources below can illicit adverse effects in at-risk individuals (celiac disease) or gluten-sensitive individuals. Even if you have never been diagnosed as being gluten sensitive, if you experience gas, stomach upset, loose bowels, stomach cramps, headache and fatigue after you eat… you may be sensitive to gluten. Identification of gluten in products can be tedious and often label reading alone is not enough. To add to the confusion, wheat-free does not always equate to gluten-free. In fact, multi-ingredient products are the most common sources of hidden gluten. Depending on the product, regulations may or may not require labeling of gluten.
What is gluten?
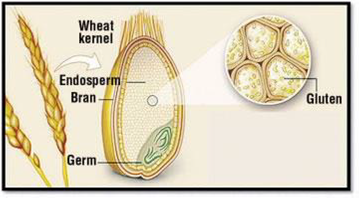
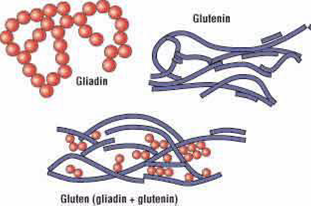
Gluten is a protein found in grains like wheat, rye and barley. It is formed from two proteins: glutenin and gliadin. The term “gluten” is derived from the glue-like consistency that arises when this protein is mixed with water. If you’ve ever kneaded bread or stretched pizza dough then you’ve seen gluten in action. Grains such as wheat, rye, barley, malt, and spelt all contain gluten. Foods made from these types of grains including pastas, breads, cereals or beer will also contain gluten. It is easy to unknowingly consume gluten from hidden sources. It hides in a wide range of foods and products.
Why do we eat wheat/gluten?
Convenience
Habit
Laziness—processed foods are convenient so they require less effort, thought, responsibility
Good taste—especially for nutrient deficient and unaware people; once you know better, you’ll avoid wheat/gluten
Government subsidization makes wheat/gluten cheap, and easily accessed by people of low socioeconomic status
Advertising
PseudoDiversity: Cereal, toast, bagel, ….sandwich, pita, …pasta, desert
Where Is Gluten Found?
Medications
Labeling standards for gluten in medications are developing. There are many prescription medications that contain excipients (that can contain gluten) to bind pills together, yet, this identification does not always happen. In general, generic versions are more likely to contain gluten. You can also ask the pharmacist or manufacturer to confirm the medication is gluten-free.
Sauces and gravies
Sauces such as soy or teriyaki typically contain wheat protein, hydrolyzed wheat starch or wheat flour. Other sauces often contain soy sauce or malt vinegar. Additionally, the base of many cream sauces and gravies is a roux, which is wheat flour mixed with butter. Get familiar with your favorite restaurants (more below) and products to ensure your sauces are gluten-free.
Starches
Wheat can be found in starches and starch derivatives. Explore the ingredient label and look for terms like “wheat starch”, “hydrolyzed wheat starch” or “contains wheat”. Wheat starch must have wheat removed to less than 20 ppm in order to be certified as gluten-free. While the term “starch” in products generally refers to cornstarch, especially in FDA regulated foods, it can also mean wheat starch. There are some gluten-free starches including tapioca starch, rice starch and potato starch.
Brown Rice Syrup
Brown rice syrup is a sweetener created by fermenting brown rice with enzymes, which break down starch to sugar. While the enzymes can be derived from fungi, they are typically from barley. This prevents the product from being gluten-free. Brown rice syrup is a stand-alone product but it is also used as an ingredient in multi-ingredient products. Some companies that use cereal enzymes will list “barley” or “barley malt” in their ingredient list. It may be difficult to verify gluten-free status in mainstream products that contain brown rice syrup as a sub-ingredient.
Soups
Companies often use wheat flour or wheat starch as a thickener for soups, which can get hidden in the ingredient label. Many soups also contain barley or other grains. Read labels carefully as pre-packaged and canned soups along with soup bases and bouillons usually contain gluten, especially those that are cream-based.
Salad dressings
Dressings can contain wheat flour, soy or malt vinegar. Many of your standard salad dressings contain wheat or gluten-containing additives like modified food starch as a thickener. Additionally, salad dressings often contain artificial colors, flavorings, dextrin, malt, soy sauce and flours that can contain gluten as a sub-ingredient. Even if the label states “wheat free”, you must still ensure there are no other gluten-containing ingredients hidden in the product.
Chips and fries
Potatoes are gluten-free; however, malt vinegar and wheat starch are often used to make potato chips. These seasonings contain gluten. Additionally, French fries are often fried in the same oil that is used to make other gluten-containing fried foods leading to cross-contamination.
Processed meats
Meat is likely the last place you’d think to look for gluten. Yet, processed meats such as preformed hamburger patties, meatballs, meatloaf, sausages and even deli meats contain gluten. Wheat-based fillers are often used in processed meats to either bind meat or improve texture. Seasoned or marinated meats often contain hydrolyzed wheat protein or soy sauce and breadcrumbs are also added to bulk up products.
Nutritional Products
How does gluten get into the nutritional products?
Minor sources: Lack of proper ventilation, filtration, and positive-pressure rooms; Lack of proper cleaning of machines between batches of products; Lack of any barrier whatsoever between processing machines—some companies have all their products being made in a single room with no barriers between machines!
Major sources: The intentional addition of buckwheat, barley and rye powder so that it creates the illusion of the vitamins/minerals/nutrients being sourced from “whole foods”—ie, they mix pharmaceutically produced vitamins with grain powder and then say the product is a whole-food product.
Restaurants: Gluten in Your Gluten-Free Foods
While gluten-free dining options have been steadily increasing, new research has elucidated that there may still be gluten in your “gluten-free” foods. While packaged foods labeled as gluten-free must contain less than 20 parts per million of gluten, there is no similar standard for gluten-free restaurant foods.
A study, published in The American Journal of Gastroenterology in March 2019, reported that a significant amount of restaurant foods classified as gluten-free contain detectable amounts of gluten. The results revealed that gluten was detected in 32% of the foods that were designated gluten-free. Interestingly, the researchers found that gluten detection differed by meal and type of food with the most gluten detection occurring at dinner and more than 50% of pizza and pasta samples testing positive for gluten.
- These results support the fact that there is gluten contamination in restaurant foods. This study highlights the prevalence of gluten contamination in restaurants and brings to light the importance of finding gluten-free menus you can trust.
Avoid glutinous grains like Wheat, Barley and Rye (the “Toxic Triad”) and replace them with Gluten-free grains like:
Quinoa Millet Certified gluten-free oats Sorghum Brown rice Buckwheat Amaranth
*You can “google” lists of gluten-free foods (just be mindful of the “hidden” ingredients described above)
What else can I do?
Take digestive enzymes containing the following:
Bromelain – A protein-digesting enzyme that helps to support digestive comfort after consumption of common food irritants. Also shown to calm inflammation that can cause stomachache.
Papain – a powerful protein-devouring enzyme – found in the papaya plant. It helps digest proteins and gluten peptides to protect you from unwanted after-meal side effects like cramping, constipation, diarrhea, bloating and gas.
Results of wheat/gluten avoidance
- Increased intake of fruits and vegetables
- Less pain and inflammation
- Weight loss
- Clearer skin
- Alleviation of…migraine, seizures, MS-like problems, autoimmunity, skin rashes including eczema and psoriasis
Dr. Larry Sharp, D.C., Associate Professor
Department of Biology
McMurry University
1 McMurry Station | # 368 | Abilene, Tx 79697
(o) 325-793-3871
Wellness Wednesday Sept 11
I am taking a short rabbit trail from the intended topic of gluten/gluten sensitivity, as this discussion occurred with a patient and my Human Anatomy & Physiology class. I will continue our exploration of gluten/gluten sensitivity next week. Thanks!
Is Your Water Bottle Making You Fat?

Summer is still with us, and everyone seems to be carrying around water. Yes, drinking water is important to our health, but some of the toxic chemicals that accompany each swig might not be. By now, we have all heard of BPA, an estrogenic compound used to make polycarbonate plastics and epoxy resins, and many people choose BPA-free plastics because of research maligning this trendy toxin with reports of infertility and genetic mutations, but do we fully understand the impact that toxins have on obesity ?
Bisphenol A (BPA), a plastics ingredient, is generally recognized as an endocrine disruptor, and concerns over its potential impact on human health have prompted manufacturers to eliminate it from some consumer products. A few nations have even implemented partial bans on how the chemical can be used, and three years ago, France went so far as to ban BPA from food packaging altogether. Yet “BPA-free” does not necessarily mean free of all bisphenols—and as a pair of recent studies show, substitutes for BPA affect cells and animals in much the same ways.
It is hard to get a handle on all the chemicals present in plastic products, no less so in items labeled BPA-free. The presumption is that at least some BPA-free items contain a BPA analog—such as bisphenol S or F (BPS, BPF)—as a replacement. INSERM’s Research Institute for Environmental and Occupational Health and the University of Rennes in France and colleagues measured the effects of four bisphenols by exposing animals (zebrafish) to high concentrations of these chemicals. The team found that three of four BPA analogs—BPS, BPF, and BPAF—are estrogenic, causing an upregulation in the brain of the enzyme aromatase, which converts androgens—such as testosterone—to estrogens. This suggests there isn’t a safe bisphenol.chemical.
A study published in Endocrinology looked instead at the influence of BPS on fat production. Exposing cell precursors extracted from women to BPA and BPS, Ella Atlas of Health Canada and colleagues found that the chemicals led the cells to accumulate lipids and differentiate into fat cells.
When it comes to weight management, the calories-in-calories-out model is outdated. The new conversation needs to shift away from treating the body like a bomb calorimeter (how we measure calories) and more like the complex biological system that it is. Plus, bomb calorimeters cannot measure how the multiplying toxins in our environment contribute to weight gain.
And they do.
The term “obesogen” was popularized by Felix Grün and Bruce Blumberg of the University of California, Irvine, back in 2006. Obesogens are considered foreign chemical compounds, or toxins, that disrupt normal development and the balance of lipid metabolism. Grün and Blumberg studied the effects of tin compounds used as fungicides, stabilizers in plastic, moluscicides and in other chemical compounds, on lipogenic, or fat-producing, activity.
Grün and Blumber’s study titled, “ Environmental obesogens: organotins and endocrine disruption via nuclear receptor signaling,” confirmed that the calories-in-calories-out model might not be the full story. They developed the environmental obesogen hypothesis that suggests xenobiotic chemicals, such as organotins and other environmental toxins, can disrupt mechanisms related to fat production and energy balance. Results showed that higher concentrations of obesogens found in the body were directly correlated to higher fat production, and also weight loss resistance. In other words, not only do obesogens contribute to obesity, they make it very difficult to lose weight even if a person is lowering calories and doing strenuous exercising .
Weight gain might be one way our bodies respond to excessive toxins. Other times, we see a breakdown in cell communication. Effective cell signaling is key to overall health, and some define disease simply as a breakdown in that cell communication. When we introduce the body to an accumulation of toxins, and studies show the average human has over 700 different toxins in the blood, cell signaling becomes is at risk for disruption. Also, the body can misinterpret toxins for biological molecules, rendering devastating health consequences, as in the case when glyphosates are mistaken for glycine.
With obesity on the rise, and more and more people complaining about being unable to lose weight, research continues to untangle the biological web that everyday toxins are weaving. Toxins, no doubt, contribute to the obesity epidemic and, with 80,000 different chemicals lurking in the environment, and 2,300 new ones being added annually, it can feel overwhelming.
Awareness, however, is the first step in changing the weight loss mindset. Rather than focusing solely on the calories-in-calories-out model, we need to change the conversation to how toxins are responsible for disrupting normal cell functioning and creating metabolic dysfunction; and we need to rethink which water bottle we are using when embarking on a weight loss program.
SO, what do I use????? Glass or stainless steel containers are preferable….NOT aluminum containers (unless you want dementia or Parkinson’s disease…..but that is another topic J…).
P.S. RECYCLED PAPER-----some of the papers being recycled and used for Napkins, Paper towels, Magazines, Store receipts, Credit card receipts, toilet paper, etc., come from magazines, credit card receipts, and other papers that are coated with plastic. Research shows that BPA is easily absorbed into the body through contact with the skin or the toxins can be transferred to your hands, and then to the food you hold and eat. I mention this because the University of Missouri-Columbia researchers conducted a human study. Non-diabetic men and post-menopausal women were orally administered a safe dose of BPA (50ug/kg body weight, an amount comparable to what they may encounter by handling cash receipts) and were compared to a control group. Results showed that the subjects receiving “safe” amounts of BPA had an altered insulin release compared to the placebo exposure.
Dr. Larry Sharp, D.C., Associate Professor
Department of Biology
McMurry University
1 McMurry Station | # 368 | Abilene, Tx 79697
(o) 325-793-3871
Wellness Wednesday Sept 4
A part of McMurry’s Wellness Task Force initiative is for health/wellness education. I would like to offer a Wellness Wednesday where a short narrative addresses some of the most current/recent topics in health education. These topics usually relate to recent questions that I have been asked in practice or related topics from class. Also, if you have a question that you would like answered, please let me know.
In several of the more popular “diets”, eating more fish (seafood) is being recommended, but there is some concern about mercury levels; therefore, to begin this weekly talk, I would like to start with seafood. The following week, I will talk about gluten/gluten sensitivity; then, options to opioids for pain; and follow this with a mini-series on CBD oils. I hope you enjoy this and please let me know if you have other topics that you want to be discussed.
Current Advice about Eating Fish

The FDA and EPA have published advice on eating fish, a protein-rich food recommended for everyone, including pregnant and breastfeeding women, women planning to conceive, and children who are 2 years and older. This resource states that eating fish may also offer heart health benefits and lower the risk of obesity.
*(FDA seafood recommendations are updated regularly. In 2017, for example, two lists of additions and changes were made to the Seafood List, including the addition of new species, such as frog and sea urchin. However, this particular resource from FDA and EPA is designed specifically for women who are or might become pregnant, breastfeeding mothers and young children.)
The 2015-2020 Dietary Guidelines for Americans recommend at least 8 ounces of seafood per week for those who consume a diet of 2,000 calories and between 8 and 12 ounces per week for women who are pregnant or breastfeeding.
The resource also states that fish are part of a healthy eating pattern and provide protein, omega-3 fats, more vitamin B12 and vitamin D than any other type of food, iron and other minerals such as selenium, zinc, and iodine.

Many people are concerned about mercury levels in fish, but the “best” and “good” choices are outlined in this resource (see table above). Two to three servings per week of the “best” choice fish are recommended, whereas just one serving of a “good” choice fish is put forth as being a healthy option. Some of the types of fish from the “best” choices include anchovies, sardines, salmon, herring, scallop, shrimp, sole, cod, and crab. “Good” choices include monkfish, halibut, carp, and yellowfin tuna. The top choices to avoid include shark, swordfish, orange roughy, marlin, king mackerel, tilefish (Gulf of Mexico) and bigeye tuna.
Dr. Larry Sharp, D.C., Associate Professor
Department of Biology
McMurry University
1 McMurry Station | # 368 | Abilene, Tx 79697
(o) 325-793-3871